
In November 2021, the American Heart Association (AHA) and the American College of Cardiology (ACC) jointly issued comprehensive guidelines for the evaluation and diagnosis of chest pain. The guidelines detail standardized risk assessments, clinical pathways, and diagnostic tools for chest pain, which provide recommendations and algorithms for clinicians to assess and diagnose chest pain in adult patients.
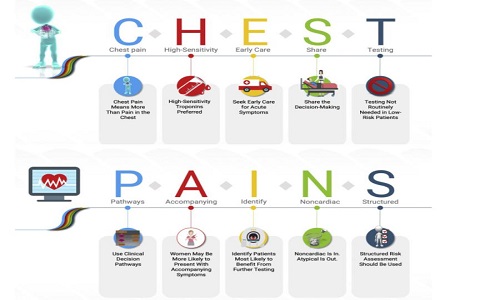
The guideline presents 10 key messages on issues and recommendations for today’s diagnostic assessment of chest pain, neatly summed up in the ten letters “chest pains”, as follows:
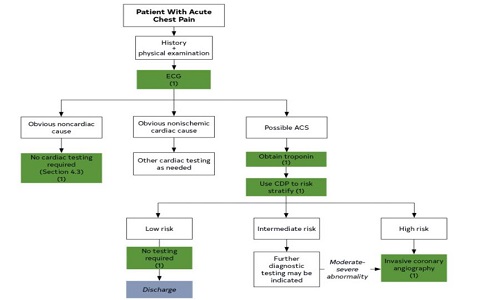
Cardiac troponin is a specific marker of myocardial cell injury and is the preferred biomarker for the diagnosis, risk stratification, treatment and prognosis of acute coronary syndromes. Guidelines combined with the use of high-sensitivity troponin, for patients with acute chest pain and suspected ACS (excluding STEMI), give the following recommendations when setting clinical decision pathways:
1.In patients presenting with acute chest pain and suspected ACS, clinical decision pathways (CDPs) should categorize patients into low-, intermediate-, and high-risk strata to facilitate disposition and subsequent diagnostic evaluation.
2.In the evaluation of patients presenting with acute chest pain and suspected ACS for whom serial troponins are indicated to exclude myocardial injury, recommended time intervals after the initial troponin sample collection (time zero) for repeat measurements are: 1 to 3 hours for high-sensitivity troponin and 3 to 6 hours for conventional troponin assays.
3.To standardize the detection and differentiation of myocardial injury in patients presenting with acute chest pain and suspected ACS, institutions should implement a CDP that includes a protocol for troponin sampling based on their particular assay.
4.In patients with acute chest pain and suspected ACS, previous testing when available should be considered and incorporated into CDPs.
5.For patients with acute chest pain, a normal ECG, and symptoms suggestive of ACS that began at least 3 hours before ED arrival, a single hs-cTn concentration that is below the limit of detection on initial measurement (time zero) is reasonable to exclude myocardial injury.
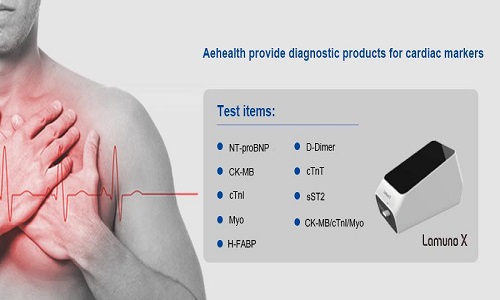
cTnI and cTnT are often used in the qualitative diagnosis of myocardial infarction, MYO is often used in the early diagnosis of myocardial infarction, and CK-MB is often used in the diagnosis of myocardial infarction after myocardial infarction. cTnI is currently the most clinically sensitive and specific marker of myocardial injury, and has become the most important diagnostic basis for myocardial tissue injury (such as myocardial infarction).AeHealth has a complete test of myocardial items, which have passed the CE certification, providing a more reliable auxiliary diagnosis basis for clinical and chest pain patients, and actively assisting the construction of chest pain centers.
Post time: Apr-02-2022